
The ability of an indirect calorimeter to accurately measure immediate and dramatic changes in gas flow and respiration gases during exercise is vital for studying bioenergetics.
Measurement of oxygen uptake (VO2) using expired gas indirect calorimetry during incremental exercise to volitional exhaustion has numerous applications in exercise physiology and clinical fields such as cardiology and pulmonology. In our previous articles, equipment-specific accuracy and variability and considerations for the use of indirect calorimeters in clinical nutrition management was discussed. While erroneous measurement of energy expenditure in the study of energetics of exercise has less deliberating results, the performance of indirect calorimetry for this purpose should not be overlooked.
Accuracy and reliability data of commercially available indirect calorimeters for the measurement of exercise energetics is limited. Furthermore, earlier research demonstrated that indirect calorimeters which accurately measures energy expenditure at rest may be less reliable for studying energetics during exercise, due to more rapid and dynamic changes in gas flow and respiration gas fractions[1, 2].
Bioenergetics of exercise
During high intensity exercise, the expired ventilation can increase from about 6 L min-1 to 200 L min-1 (or even > 220 L·min-1 in elite athletes), with a corresponding maximum VO2 and carbon dioxide produced (VCO2) of 2.7 to 7.0 L·min-1 (or >7.0 L·min-1) in men in short periods of time[2, 3].
Reliable measurements of ventilation and expired gas fractions, especially, ascertain accurate energetic costs or determinants of VO2 during exercise[4]. However, establishing the accuracy and validity of measurements using expired air indirect calorimetry is difficult as there is no standardized methodology that simulates respiration patterns during various exercise activities. A study using a metabolic simulator over four increases in ventilation found larger measurement deviations in mean expiratory flow, oxygen uptake (VO2), carbon dioxide production (VCO2) and respiratory exchange ratio (RER; ratio of oxygen uptake and carbon dioxide produced) at higher ventilations[1]. Similarly, the same study showed that reliability of measurements at exercise intensities up to 150W differed between indirect calorimeters, with coefficient of variation ranging from 3.3-7.0%, and even up to 45.8%[1].
VO2max measurement
The maximum rate of oxygen consumption (VO2max) or aerobic capacity, defined as the highest rate at which oxygen can be taken up, transported and utilized by the body for producing energy is used as an example for discussion. As VO2max is used to assess cardiopulmonary and metabolic systems, obtaining valid and reliable data is of great interest and importance. Howley et al. [4] estimated that ideally, an error of not more than ±2% should be contributed by expired gas analysis indirect calorimetry for the measurement of VO2max. Greater measurement error and variability at higher ventilations is especially undesirable for studying exercise physiology. The range of relative VO2max, expressed as O2 per kilogram of body weight per min, is generally about 65 – 85 mL·kg-1·min-1 in endurance runners/cyclists, 45 – 65 mL·kg-1·min-1 in non-endurance athletes (e.g. football players, basketball players), and 25 – 45 mL·kg-1·min-1 in college-aged non-athletes[2]. The highest value recorded is 94 mL·kg-1·min-1 in a male cross-country skier.
Example:
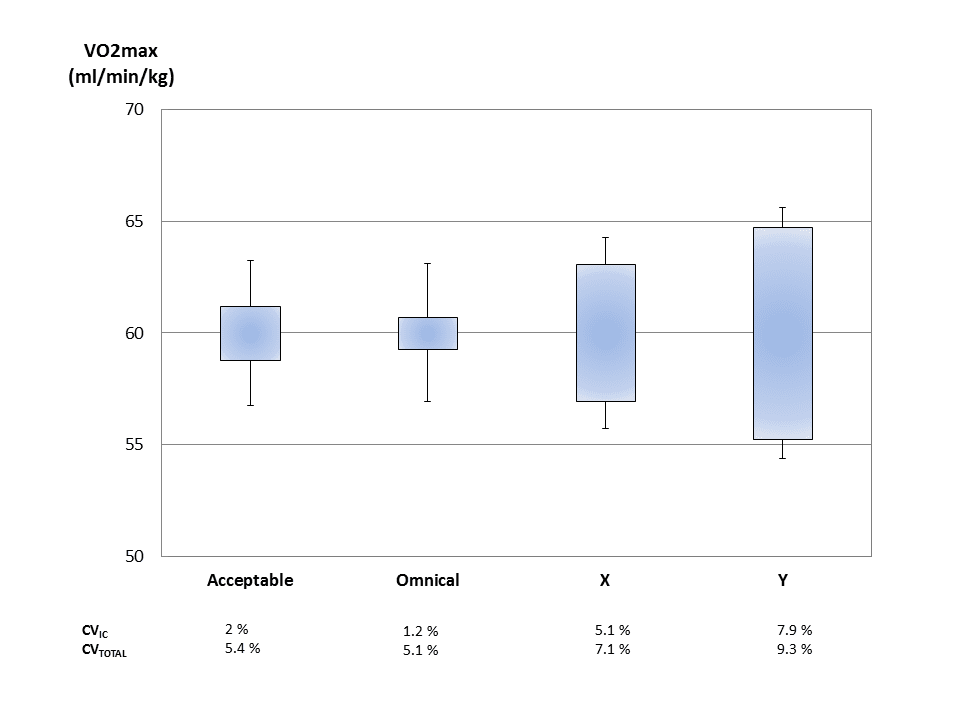
For an adult athlete with a mass of 75kg and VO2max of 60 mL·kg-1·min-1 and corresponding VO2 of 4.5 L·min-1, the graph on the right illustrates the dispersion around the actual VO2max value measured using different indirect calorimeters (Omnical, Instrument X and Instrument Y with reported CVs for VO2max (+/-SD) taken from published literature[1]), in comparison to acceptable variation. CVIC : Box graphs show the range of measurements due to instrumental variation; CVTOTAL : high/low bars show the total variation due to instrumental and biological variation.
A coefficient of variation (CVIC) of 2% due to instrumental variation corresponds to a standard deviation of 1.2 mL·kg-1·min-1 or 0.090 L·min-1. Since the biological variability in VO2max is about 5%[5], the total coefficient of variation, CVTotal = (52 + 22)1/2 = 5.4%, total standard deviation of ±2.7 mL·kg-1·min-1 (range of 56.8 – 63.2 mL·kg-1·min-1) and corresponding ±0.150 L·min-1 in VO2 is likely.
A CVtotal of 5.4% or more can contribute to a sizeable error of measurement of VO2max, with considerations to the expected magnitude of change or trainability. Conservative improvements of 5.5 and 7.2% in VO2max have been observed in moderately-trained endurance runners with an initial VO2max of 55.5 to 60.5 mL·kg-1·min-1 after eight weeks of exercise training interventions[6]. Similarly, another study observed an increase in VO2max of 10.3%, from 66.6 mL·kg-1·min-1 following one year of training program in elite endurance cyclists [7]. Therefore, to ascertain if the magnitude of change in VO2max observed is true, it is imperative that the measurements are accurate and instrument variation is low.
Comments
With the above considerations, it is deduced that expired gas indirect calorimeters should be validated for the full range of technical and biological variability. Testing at physiological range of O2 consumption and CO2 production from resting to elite athlete levels using methanol combustion simulating resting metabolic rate and gas infusions simulating a range of higher physiological limits are well-accepted methods for validation. Test-retest variability of individual instruments is also necessary for validation of repeatability of measurements.
The Omnical (Maastricht Instruments B.V.) achieved a high degree of technical validated accuracy over the full physiological range (0.44 ± 0.75% for VO2 and -0.11 ± 1.05% for CO2 over the 500 – 6000 mL.min-1 infusion range) and exceptional repeatability with a mean within-subject CV for VO2max of 1.2% (results not yet published). It is essential to choose an instrument with excellent accuracy and reliability to ensure valid results and to have confidence in measurements. Maastricht Instruments supplies the Omnical system that allows researchers to easily conduct various studies.
Contact us for more information.
References
- Carter, J. and A.E. Jeukendrup, Validity and reliability of three commercially available breath-by-breath respiratory systems. Eur J Appl Physiol, 2002. 86(5): p. 435-41.
- Boone, T., Introduction to exercise physiology. 2014, Burlington, MA: Jones & Bartlett Learning. xliii, 532 p.
- Gore, C.J., et al., Automated VO2max calibrator for open-circuit indirect calorimetry systems. Med Sci Sports Exerc, 1997. 29(8): p. 1095-103.
- Howley, E.T., D.R. Bassett, Jr., and H.G. Welch, Criteria for maximal oxygen uptake: review and commentary. Med Sci Sports Exerc, 1995. 27(9): p. 1292-301.
- Katch, V.L., S.S. Sady, and P. Freedson, Biological variability in maximum aerobic power. Med Sci Sports Exerc, 1982. 14(1): p. 21-5.
- Helgerud, J., et al., Aerobic high-intensity intervals improve VO2max more than moderate training. Med Sci Sports Exerc, 2007. 39(4): p. 665-71.
- Storen, O., et al., Improved VO2max and time trial performance with more high aerobic intensity interval training and reduced training volume: a case study on an elite national cyclist. J Strength Cond Res, 2012. 26(10): p. 2705-11.